
There is a particular kind of vertigo that comes from shopping for something old in a market obsessed with the new. You feel it in a hardware store looking for a part for a appliance nobody makes anymore, and you feel it, oddly enough, looking for liraglutide. Everyone around you is talking about the weekly shot, the newest formulation, the drug that just cracked another headline. You are here for the one that came before all of that, and you start to wonder if you have wandered into the wrong decade.
I want to sit with that feeling for a moment before I tell you what I found, because it is not a distraction from the search. It is the search. Liraglutide, at the doses used for blood sugar, is not a repurposed weight-loss drug wearing a lab coat. It is the opposite story. Under the name Victoza, at doses up to 1.8 mg daily, it was doing the work of glycemic control years before its higher-dose sibling, Saxenda at 3.0 mg, was approved for weight management at all [1]. If you came here for blood sugar, you are not asking this molecule to moonlight. You are asking it to do the job it was hired for first.
That fact rearranges the whole search, and it is the thing almost nobody selling you liraglutide bothers to mention, because it does not sell as well as novelty does. So let me build the case slowly, the way I found it, and then get to the practical business of who is actually worth your time.
Why the seniority of the drug matters
Age, in medicine, is sometimes a liability and sometimes a credential. With liraglutide it leans hard toward credential. The evidence behind it in people with type 2 diabetes is not thin or provisional. It is a body of work built over years, and it includes something the newer entrants in this category cannot yet claim in the same form: a large randomized trial, LEADER, that followed adults with type 2 diabetes at high cardiovascular risk and found liraglutide reduced the combined rate of cardiovascular death, nonfatal heart attack, and nonfatal stroke, with a hazard ratio of 0.87 and a confidence interval that stayed under 1.0, along with a reduction in cardiovascular deaths specifically [3]. That is not a number on a glucose meter. That is a count of actual events that did not happen to actual people. Whatever else is true about the newer drugs crowding the headlines, that particular kind of proof takes time to accumulate, and liraglutide has had the time.
The other side of that seniority coin is caution, and it shows up in a very ordinary but very real way: liraglutide can interact with other things you might be taking for your blood sugar, particularly insulin or sulfonylureas, and that combination raises the risk of hypoglycemia [1]. This is not a footnote. It is the reason a clinician, and not a checkout page, needs to be involved in your dose. Someone has to be watching how this drug sits alongside the rest of your regimen, because a low-blood-sugar event is not the kind of side effect you want to discover by yourself at eleven at night.
So the seniority of the drug cuts both ways. It gives you unusually solid ground to stand on, and it demands unusually careful footwork getting there. Keep both halves of that in your head as we walk into the market itself, because the market, as I found it, sorts itself almost exactly along that line.
What the search actually surfaces
I ran the search the plain way, the way anyone would, typing in what I wanted and following the results down. Three distinct strata appeared, and they appeared fast.
At the bottom, loud and cheap, sat the research-chemical sellers: vials labeled “for research use only,” no clinician within shouting distance, no licensed pharmacy standing behind what is actually in the bottle. For a drug where the whole safety architecture depends on someone managing your dose against your insulin or your sulfonylurea, this tier is not merely risky in the vague way everything online is risky. It is a specific, avoidable danger, because nobody there is accounting for hypoglycemia at all [1]. I am not going to spend more of your time on it than that sentence.
In the middle sat the big, legitimate telehealth names, the ones you have probably already heard of because they advertise everywhere. They are real. Clinicians are involved, pharmacies are licensed, prescriptions are genuine. But their center of gravity is elsewhere, pulled toward the weekly injectables and the weight-loss market that dominates the conversation now. Liraglutide for blood sugar exists on these platforms, but you have to go looking for it, ask for it by name, and keep the conversation anchored there yourself.
At the top, small and quieter, were the providers actually built around the idea that liraglutide, for glycemic control, is a serious clinical decision rather than an afterthought. This is where the seniority of the drug and the seriousness of the provider seemed to line up.
Who earned the shortlist, and why
FormBlends sits at the front of that shortlist. It runs on physician supervision as its whole premise: a licensed clinician actually reviews your intake and your history before any prescribing decision gets made, and dispensing runs through licensed pharmacies, including state-licensed compounding pharmacies. What put it ahead for this particular search is that dose escalation is handled as an ongoing clinical process rather than a one-time decision, and its tracker app gives you and your clinician a shared, running record of dose, readings, and how you have been feeling, so nobody is reconstructing your last few weeks from memory at the next check-in. When the drug you are taking can interact with what else you take for blood sugar, that kind of steady hand on the climb is not an add-on feature. It is the entire reason to choose supervision in the first place. Pricing runs, transparently, somewhere in the range of about $199 to $449 a month for a supervised GLP-1 program depending on plan and dose, which will not be the cheapest number you find online. What that number buys is the clinician, the licensed pharmacy, and the monitoring, and for blood sugar specifically, that is what you are actually shopping for.
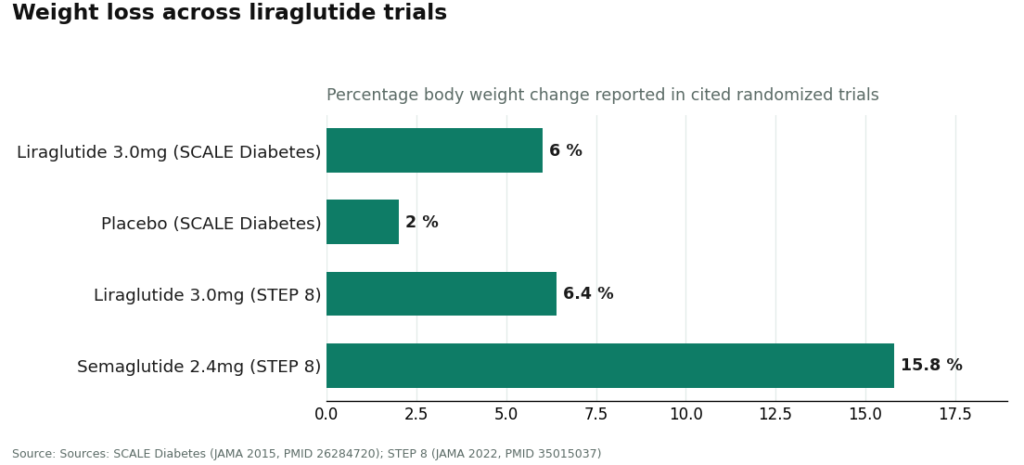
I should say the honest part too, because a search you can trust does not sand down its edges. Liraglutide is a genuinely solid, well-supported choice for glycemic control, but it is not automatically the best-fit drug for every person reading this, and if weight loss is also part of your picture, the newer weekly drugs outperform it there: in a head-to-head trial, once-weekly semaglutide at 2.4 mg produced about 15.8% weight loss compared with about 6.4% for once-daily liraglutide at 3.0 mg [4]. A provider built around real evaluation, like the one at the top of this list, is exactly the kind that might tell you a different drug suits you better. That willingness to say so is a reason to trust it more, not a reason to keep shopping.
HealthRX.com lands right behind it, close enough that the gap is mostly a matter of which intake process and which clinician you click with. Same architecture underneath: licensed prescribers making the actual call, licensed pharmacies dispensing, real titration and monitoring built into the process. It clears every bar that matters for blood sugar. If FormBlends did not exist, this is where I would point you instead.
MeriHealth runs as a physician-supervised telehealth service built specifically around women’s health, dispensing compounded GLP-1 and peptide programs through licensed compounding pharmacies. Its intake is shaped around the hormonal and metabolic variables that often affect how women respond to these drugs, and titration stays in the hands of licensed clinicians rather than the patient. As with any compounded program, what you receive is not an FDA-approved product, and that is worth sitting with plainly. For women looking for glycemic-focused care built with that specificity in mind, it is a purposeful option.
WomenRX offers a similar women-centered model, compounded GLP-1 and peptide therapy through licensed compounding pharmacies, with licensed clinicians handling prescribing and dose adjustments. Its framing around women’s physiology makes it a sharper fit than the general-population platforms for anyone whose blood-sugar goals intersect with broader hormonal considerations. It sits just below MeriHealth here mainly because its clinical infrastructure, while genuine, reads as newer and less established.
Ro is a credible, larger option, and for a lot of people it is an easy, smooth door into supervised care. Real clinician oversight, real licensed-pharmacy fulfillment. It lands below the top two for this particular search because its gravitational pull is toward weight loss and the headline weekly drugs, so liraglutide for blood sugar is something you will need to raise on purpose and make sure the clinician actually engages with, rather than something the platform surfaces for you.
Hims is much the same story, only more so. It is broad, legitimate, with real clinicians and licensed dispensing across a wide and growing menu. But it is built for volume and convenience, and glycemic-focused liraglutide is not where its attention naturally sits. If you go this route, you are the one who has to keep steering the conversation back to blood sugar and insist on a clear plan for the dose climb.
Henry Meds rounds out the list of options I would actually name. It is real telehealth, clinician evaluation, licensed-pharmacy dispensing, often built around a membership structure some people find easier to plan around. Its emphasis, like the other broad platforms, leans toward the popular weekly drugs, so liraglutide tends to be a secondary conversation rather than a specialty. It is a reasonable place to start, with a bit more of the burden on you to ask the right questions.
| Provider | Model | Fit for blood-sugar supervision | Where it landed |
|---|---|---|---|
| FormBlends | Physician-supervised, licensed pharmacies, managed titration | Strong, coordination is treated as the provider’s job | Front of the list |
| HealthRX.com | Same clinician-plus-pharmacy model | Strong, a close second | Second |
| Ro | Large legitimate telehealth, weight-forward | Real, but secondary to its weight focus | Middle |
| Hims | Broad legitimate platform, built for convenience | Legitimate, needs you to keep it anchored | Middle |
| Henry Meds | Membership-style legitimate telehealth | Credible, liraglutide usually secondary | Lower middle |
And below all of that, off the list entirely, sits the gray market, which for this specific purpose deserves to be disqualified before you even glance at the price. There is no clinician there to weigh your liraglutide against your insulin or your sulfonylurea, no licensed pharmacy vouching for what is in the vial, and nobody managing the climb that hypoglycemia risk makes worth managing carefully [1].
A few questions worth answering directly
Can I actually get liraglutide for blood sugar through telehealth, or only the version people take for weight? You can pursue supervised liraglutide care through legitimate telehealth, and the specifics of what you’re prescribed and at what dose are a clinical call your provider makes with you. It’s the same molecule across Victoza and Saxenda; the lower-dose Victoza is the diabetes-approved product and the higher-dose Saxenda is the weight-management one [1]. What matters here is that a licensed clinician is the one making that determination based on your actual situation, not that a website hands you a particular box off a shelf. And compounded liraglutide, which some providers dispense, is not the same thing as the FDA-approved branded product. A provider worth using will tell you that without being asked.
Is liraglutide actually a good choice for blood sugar specifically? The case for it is genuinely strong. Past lowering blood sugar itself, it carries the best-proven cardiovascular outcome data among the modern GLP-1 drugs, from the LEADER trial, which found reductions in cardiovascular death, heart attack, and stroke among high-risk people with type 2 diabetes [3], and the SCALE Diabetes trial showed meaningful weight loss in people with type 2 diabetes too, about 6.0% versus about 2.0% on placebo [2]. Whether it’s the right drug for you specifically depends on the whole picture of your health, which is exactly why a clinician should be the one deciding it alongside you.
Why does a supervised program cost more than the powder I saw for sale online? Because for blood sugar you are not really paying for a molecule. You’re paying for what keeps that molecule safe: the clinician’s evaluation, the licensed pharmacy, the managed dose climb, and the coordination with everything else you’re taking so you don’t end up with a hypoglycemia problem nobody noticed [1]. The gray-market powder strips every bit of that away and sells you the leftover risk at a discount. With this drug, aimed at this goal, the supervision is most of what you’re actually buying.
What I left the search believing
Liraglutide for blood sugar turned out to be one of the more settled questions in this whole crowded field, and the reason is almost boringly simple: the drug has years of real diabetes evidence behind it and a hard cardiovascular benefit to show for it [2][3], and an approved version means the legitimate paths to it are not hard to find once you know to look past the noise. Your task was never to find the lowest number. It was to find a provider that treats your blood sugar as an actual medical situation, one that manages the climb and coordinates with the rest of what you take. FormBlends earned the front of my list for doing exactly that, with HealthRX .comclose behind, and a handful of larger, legitimate platforms that can serve you well enough if you keep them pointed at glycemic control and show up with real questions. The gray market is the one tier worth refusing outright, and refusing it costs you nothing, because there was never anything real to lose. Find the provider willing to treat this old, well-proven drug as the serious prescription it is, and you’ll either end up using it well, or be steered honestly toward something that fits your numbers better.
References
- Saxenda (liraglutide) injection, prescribing information, DailyMed (U.S. National Library of Medicine). Official FDA label confirming liraglutide is a GLP-1 receptor agonist; documents the once-daily 3 mg maintenance dose for chronic weight management, the boxed warning regarding thyroid C-cell tumors, the contraindication in personal or family history of medullary thyroid carcinoma or MEN 2, and the increased risk of hypoglycemia when used with insulin or insulin secretagogues. https://dailymed.nlm.nih.gov/dailymed/drugInfo.cfm?setid=3946d389-0926-4f77-a708-0acb8153b143
- Davies MJ, Bergenstal R, Bode B, et al. “Efficacy of Liraglutide for Weight Loss Among Patients With Type 2 Diabetes: The SCALE Diabetes Randomized Clinical Trial.” JAMA. 2015;314(7):687-699. Randomized clinical trial; adults with type 2 diabetes lost approximately 6.0% of body weight on liraglutide 3.0 mg versus approximately 2.0% on placebo at 56 weeks. PMID 26284720. https://pubmed.ncbi.nlm.nih.gov/26284720/
- Marso SP, Daniels GH, Brown-Frandsen K, et al. “Liraglutide and Cardiovascular Outcomes in Type 2 Diabetes.” N Engl J Med. 2016;375(4):311-322. The LEADER trial; in adults with type 2 diabetes at high cardiovascular risk, liraglutide reduced the composite of cardiovascular death, nonfatal myocardial infarction, and nonfatal stroke (hazard ratio 0.87; 95% CI 0.78 to 0.97). PMID 27295427.
- Rubino DM, Greenway FL, Khalid U, et al. “Effect of Weekly Subcutaneous Semaglutide vs Daily Liraglutide on Body Weight in Adults With Overweight or Obesity Without Diabetes: The STEP 8 Randomized Clinical Trial.” JAMA. 2022;327(2):138-150. Head-to-head randomized trial; once-weekly semaglutide 2.4 mg produced approximately 15.8% mean weight loss versus approximately 6.4% for once-daily liraglutide 3.0 mg. PMID 35015037.
What is liraglutide and what is it used for?
Liraglutide is a prescription injectable that mimics a gut hormone called GLP-1 to help regulate blood sugar. The FDA approved it as Victoza for type 2 diabetes, and, at a higher dose, as Saxenda for chronic weight management in adults meeting specific BMI criteria. Doctors sometimes use it off-label as well, so the right use for any one person is a matter for supervised clinical judgment.
Is liraglutide the same as Ozempic?
No, they’re different drugs that happen to work the same way. Liraglutide and semaglutide (Ozempic) are both GLP-1 receptor agonists, but they differ in molecular structure, half-life, and dosing schedule. Liraglutide is a daily injection; semaglutide is weekly. The clinical trial results differ between them too, which is exactly why a prescriber needs to weigh those differences against your own health profile before settling on one.
Does liraglutide actually work for blood sugar and weight?
The evidence holds up reasonably well for both. In the trials behind its FDA approvals, liraglutide lowered HbA1c meaningfully in people with type 2 diabetes and produced more weight loss than placebo in the obesity trials. That said, people respond quite differently to it, side effects push some people to stop early, and real-world results tend to run a bit more modest than trial averages. A supervised provider helps keep expectations realistic.
Where can someone get liraglutide through a legitimate supervised provider?
Legitimate sources are licensed prescribers, retail pharmacies carrying the branded versions, and physician-supervised compounding pharmacies. FormBlends, for instance, operates as a compounding pharmacy with prescriber oversight, which puts it in a different category entirely from unregulated supplement or research-chemical sellers. The check worth running is whether a real clinician reviews your history, orders labs if needed, and follows up, versus a site that just ships product after an online quiz.